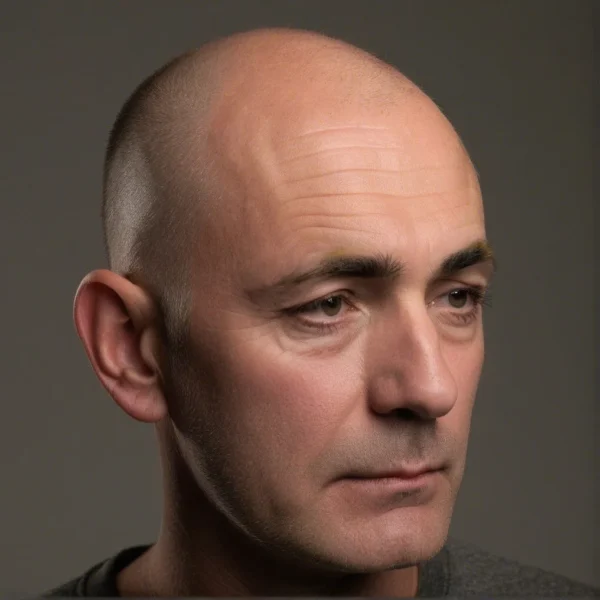
The Sign of Hertoghe, also known as Queen Anne’s sign, refers to the thinning or loss of the lateral third of the eyebrows. Although once used diagnostically for identifying hypothyroidism, it is now recognized in various contexts, including nutritional deficiencies, dermatological conditions, and other hormone-related conditions. This article reviews the historical context, epidemiology, clinical significance, pathophysiology, and management of the Sign of Hertoghe, with an emphasis on its use as a clinical clue. Additionally, we explore its differential diagnosis, which ranges from alopecia areata to other inflammatory disorders. A deeper understanding of this clinical sign can lead to early recognition and appropriate treatment of underlying conditions.
Introduction: The human eyebrow serves several physiological, protective, and expressive functions, playing a significant role in facial aesthetics and nonverbal communication. In medical practice, certain eyebrow changes can provide important clues to underlying disease processes. One such clue, referred to as the Sign of Hertoghe or Queen Anne’s sign, is characterized by the selective thinning or loss of the outer portion of the eyebrows. While historically associated most strongly with hypothyroidism, the Sign of Hertoghe also appears in a variety of other conditions, including several dermatological diseases, nutritional deficiencies, and allergy-related conditions.
Historical Background: The Sign of Hertoghe owes its name to Dr. Eugene Hertoghe, a Belgian physician who practiced in the late 19th and early 20th centuries. His work largely focused on thyroid gland physiology and disorders, including hypothyroidism and myxedema. Dr. Hertoghe observed that many patients with underactive thyroid glands exhibited a peculiar thinning of the eyebrow at its lateral aspect (the outer edge or “tail” of the eyebrow). This observation later gained prominence in medical circles, leading to the sign being widely cited as a hallmark clinical feature of hypothyroidism.
The name “Queen Anne’s sign” emerged from a historical anecdote that Queen Anne of Denmark (1574–1619), wife of King James I, allegedly displayed characteristic eyebrow changes. Although corroborating medical evidence is limited, this eponym persisted in historical medical texts, lending color to the descriptive nomenclature. Over time, with advancements in laboratory diagnostics, the Sign of Hertoghe lost some of its original diagnostic specificity for hypothyroidism as clinicians discovered this sign in other diseases as well. Despite its broadening context, the name “Sign of Hertoghe” remains firmly entrenched in the medical lexicon.
Epidemiology and Clinical Significance: While no large-scale epidemiological studies exist that capture the exact prevalence of the Sign of Hertoghe in the general population, hypothyroidism remains one of the most common endocrine disorders worldwide, and the eyebrow changes may be encountered in a subset of hypothyroid patients. Additionally, dermatologists observe that eyebrow thinning can occur in individuals with chronic skin conditions or nutritional imbalances. Taken collectively, these factors indicate that the Sign of Hertoghe is not a rare finding, though its prevalence in specific patient populations is likely variable.
The clinical significance of the Sign of Hertoghe rests on its potential utility as a red flag for underlying systemic disease. Whereas the thinning of eyebrows might be dismissed as a cosmetic or age-related change, proper appreciation of this sign can prompt further evaluations, ultimately leading to earlier diagnosis of conditions such as hypothyroidism, atopic dermatitis, or even specific nutritional deficiencies (e.g., essential fatty acid deficiency). In an era of specialized diagnostics and imaging, the importance of simple clinical observation should not be understated.
Etiopathogenesis: The etiopathogenesis of lateral eyebrow thinning is multifactorial and reflects a variety of underlying pathological processes. Below are some of the most common etiological categories:
Endocrine Dysfunction
Hypothyroidism: Reduced thyroid hormone levels lead to a slowed hair growth cycle, hair thinning, and changes in hair texture. The eyebrow, already predisposed to sparser hair density toward its lateral aspect, can be preferentially affected.
Hypopituitarism: In panhypopituitarism, deficiency in thyroid-stimulating hormone (TSH) and/or other pituitary hormones can induce hair loss that includes the eyebrows.
Nutritional Deficiencies
Protein Deficiency: Hair is a protein filament, and insufficient dietary protein intake can result in weakened hair shafts and reduced hair growth.
Essential Fatty Acids and Micronutrient Deficiencies: Certain micronutrients (iron, selenium, zinc) and essential fatty acids support normal hair cycling. Deficiencies in these nutrients have been tied to various forms of hair loss.
Dermatological and Autoimmune Conditions
Atopic Dermatitis: Chronic inflammation and scratching can lead to mechanical loss of eyebrow hair as well as damage to hair follicles.
Alopecia Areata: An autoimmune condition that commonly involves the scalp but can affect eyebrows in patchy, nonscarring hair loss.
Psoriasis: In some cases, psoriatic plaques around the hairline or eyebrows can disrupt hair growth.
Inflammatory and Infectious Causes
Chronic Inflammatory Disorders: These can damage follicles or alter hair cycling, resulting in eyebrow thinning.
Leprosy: Historically, eyebrow loss is noted as a feature of lepromatous leprosy, particularly in untreated cases.
Aging
With advancing age, hair density naturally decreases, and eyebrow hair may become thinner or coarser. While this is a normal aging process, it can be mistaken for pathological signs if abrupt changes occur.
Thus, the variety of potential etiologies underscores the need for a careful patient workup. Clinicians must assess dietary, endocrine, and dermatological factors when faced with lateral eyebrow thinning.
Clinical Presentation and Examination: The hallmark clinical presentation of the Sign of Hertoghe is the progressive loss of hair along the lateral portion of the eyebrow, often affecting the outer third. The patient or clinician might first note a subtle decrease in eyebrow thickness. Over time, this thinning may progress until that portion of the eyebrow appears nearly absent. Occasionally, the same phenomenon can begin medially or around the midpoint of the eyebrow, but lateral thinning is by far the most common.
On clinical examination, a dermatologist or primary care physician should assess not only the eyebrows but also the scalp and body hair to evaluate whether the thinning is isolated or part of a generalized hair loss process. An important aspect is to look for signs of mechanical hair loss such as breakage or friction damage. Additionally, assessing the skin integrity, noting any eczematous lesions, scaling, or evidence of infection, can further guide the diagnosis.
Standard investigations often include thyroid function tests (TSH, free T4, and sometimes free T3), particularly if there are accompanying symptoms suggestive of hypothyroidism such as weight gain, cold intolerance, or fatigue. Serum levels of iron, ferritin, zinc, and other micronutrients may also be checked. In selected cases, clinicians may perform a skin scraping or biopsy if inflammatory or autoimmune conditions are suspected.
Differential Diagnosis: Various conditions can mimic or contribute to the appearance of lateral eyebrow thinning. Important differential diagnoses include:
Alopecia Areata: This autoimmune condition can cause patchy hair loss in the scalp and eyebrows. When it selectively involves the lateral eyebrow, it can resemble the Sign of Hertoghe. A key difference is that alopecia areata often presents as discrete, well-demarcated patches and may be associated with exclamation point hairs.
Trichotillomania: In some patients, conscious or subconscious pulling of eyebrow hair can lead to thinning that is sometimes lateral-predominant. Careful history taking and inspection of the hair shafts can help differentiate this from systemic causes.
Atopic Dermatitis: Chronic rubbing or scratching due to pruritus can cause mechanical hair loss around the eyebrow margins. Signs of eczematous dermatitis on or around the face can often provide diagnostic clues.
Aging: While typically symmetrical, progressive thinning of the eyebrows with age can mimic this sign. Historical documentation of the speed of hair loss can often distinguish typical aging from pathological processes.
Recognizing these conditions is crucial to avoid anchoring bias, in which clinicians may prematurely conclude hypothyroidism based on the Sign of Hertoghe alone. A thorough clinical history, physical examination, and targeted investigations remain paramount.
Associated Conditions: Though hypothyroidism remains the prototypical cause associated with the Sign of Hertoghe, a variety of other conditions have been reported in the medical literature:
Primary Hypothyroidism: May be caused by Hashimoto’s thyroiditis, iodine deficiency, or thyroidectomy. In Hashimoto’s thyroiditis, thinning of the lateral eyebrows may be accompanied by a range of thyroid-related signs and symptoms.
Secondary Hypothyroidism (Hypopituitarism): Lower TSH production due to pituitary dysfunction can cause changes identical to those in primary hypothyroidism.
Atopic Dermatitis: Here, the hair loss may be attributed to inflammation and mechanical forces.
Nutritional and Metabolic Disorders: Chronic malnutrition, or specific deficiencies in iron or essential fatty acids, can contribute to eyebrow hair loss.
Systemic Lupus Erythematosus (SLE): While less common, patients with SLE may develop non-scarring hair loss involving the scalp or eyebrows due to systemic inflammation.
Management: Management of the Sign of Hertoghe is twofold: addressing the underlying cause and providing supportive therapies. The mainstay of treatment is correction of the underlying pathology—most commonly thyroid hormone replacement in patients with confirmed hypothyroidism.
Thyroid Hormone Replacement: In hypothyroid patients, restoration of normal thyroid hormone levels with levothyroxine often results in significant improvement in hair texture and eyebrow regrowth, although this process can take several months. Achieving a euthyroid state is crucial for hair follicle cycling to normalize.
Nutritional Support: Correcting deficiencies in iron, zinc, and other micronutrients can help stimulate hair regrowth. A balanced diet with adequate protein, vitamins, and essential fatty acids is recommended. In some instances, supplementation might be necessary.
Topical Treatments: For inflammatory conditions like atopic dermatitis or psoriasis, topical corticosteroids, calcineurin inhibitors, or other anti-inflammatory therapies can help reduce inflammation and facilitate eyebrow regrowth.
Behavioral Interventions: If mechanical factors such as trichotillomania are contributing, cognitive-behavioral therapy, habit reversal training, or stress management techniques may be beneficial.
Cosmetic Solutions: In cases where eyebrow regrowth is slow or incomplete, cosmetic options such as eyebrow pencils, microblading, and eyebrow transplantation can be considered to restore a natural appearance.
Prognosis: The prognosis for the Sign of Hertoghe largely depends on the underlying cause. In patients with hypothyroidism, appropriate and timely treatment often leads to improvement in eyebrow hair density within a few months, though complete restoration can vary among individuals. For inflammatory causes like eczema or psoriasis, controlling the inflammation may facilitate partial to complete regrowth, provided that there is no permanent follicular damage. Situations involving longstanding nutritional deficiencies also typically respond positively once deficiencies are corrected.
However, in certain chronic autoimmune conditions (e.g., alopecia areata) or scarring processes, the extent of hair regrowth can be unpredictable. Early identification remains crucial for optimizing outcomes, underscoring the importance of vigilance in clinical examination.
Conclusion: The Sign of Hertoghe, or Queen Anne’s sign, remains a pertinent clinical observation despite modern diagnostic tools. Characterized by the thinning or loss of the lateral third of the eyebrows, it may initially suggest hypothyroidism but also encompasses a broad differential diagnosis, including nutritional disorders, inflammatory dermatological conditions, and autoimmune diseases. Accurate recognition and assessment of this sign can guide clinicians to an underlying diagnosis that, once addressed, can often reverse or ameliorate the hair loss.
In an increasingly specialized and technology-driven medical landscape, the Sign of Hertoghe serves as a reminder of the value of meticulous observation and physical examination. While laboratory evaluations and imaging studies play a key role in contemporary practice, they cannot replace the astute eye of the physician. Clinical signs such as lateral eyebrow thinning are early indicators that can hasten diagnosis and improve patient outcomes when recognized promptly. Ongoing research into the pathophysiology of hair follicle biology will further clarify the mechanisms involved, opening up new avenues for preventing and treating eyebrow thinning.
Ultimately, the enduring significance of the Sign of Hertoghe in clinical medicine is testament to the importance of simple, yet powerful bedside observations. By retaining an appreciation for these classical physical findings, practitioners can continue to deliver comprehensive, patient-centered care—a balance of tradition and modern science that lies at the heart of effective medical practice.
Polemann G, Peltzer L. [The eye brow sign of Hertoghe, a symptom of function of the autonomic nervous system]. Medizinische. 1952 Jun 21;31(25):856–60.
1.
Lane Furdell E. Eponymous, anonymous: Queen Anne’s sign and the misnaming of a symptom. J Med Biogr. 2007 May;15(2):97–101.
1.
Tanei R, Katsuoka K. Clinical analyses of atopic dermatitis in the aged. J Dermatol. 2008 Sep;35(9):562–9.
1.
Kumar KVSH, Prusty P. Visual vignette. The Hertoghe sign. Endocr Pract. 2011;17(4):666.
1.
Parrino D, Di Bella S. Hertoghe sign: a hallmark of lepromatous leprosy. QJM. 2016 Jul;109(7):497.
1.
Ashrafian H. Hypothyroidism in the “Arnolfini Portrait” (1434) by Jan Van Eyck (1390-1441). J Endocrinol Invest. 2018 Jan;41(1):145–7.
1.
Borzutzky A, Tejos-Bravo M, Venegas LF, Iturriaga C. Hertoghe’s Sign in Atopic Dermatitis. J Pediatr. 2020 Nov;226:299.
1.
Kobylianskii J, Gold WL. Queen Anne sign. CMAJ. 2022 Feb 14;194(6):E219.
1.
Taguchi H, Nishioka H. Eyebrow loss and the Queen Anne sign in hypothyroidism. QJM. 2023 Dec 27;116(12):1029–30.
Scalp psoriasis is a chronic, noncontagious skin condition that predominantly affects the scalp, manifesting in scaly, red, and raised patches. This condition can extend beyond…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.