Introduction: Folliculitis is a common dermatological condition characterized by the inflammation of hair follicles. It manifests as small red or pus-filled bumps around hair follicles, often resembling acne or a skin rash. Folliculitis can occur anywhere on the body where hair is present, but it most commonly affects areas that are prone to friction, such as the scalp, face, chest, back, buttocks, and thighs. While it is generally a benign and self-limiting condition, folliculitis can cause discomfort, itching, and, in severe cases, lead to skin scarring or permanent hair loss. This article provides an overview of the clinical features, etiology, and management strategies for folliculitis, focusing on its different forms, causes, and treatment options.
Clinical Features of Folliculitis: The clinical presentation of folliculitis can vary depending on the type of folliculitis and its underlying cause. In general, the hallmark of folliculitis is the presence of small, erythematous papules or pustules centered around hair follicles. Other common symptoms include:
Itching or burning sensation: Many individuals experience pruritus (itch sensation) or discomfort in the affected areas.
Pain or tenderness: In more severe cases, the lesions may become painful or tender to the touch.
Pustules or papules: Small, pus-filled lesions often develop around the hair follicles, sometimes progressing into larger nodules or abscesses.
Crusting: In some cases, the pustules may rupture, leading to crusting or scabbing of the skin.
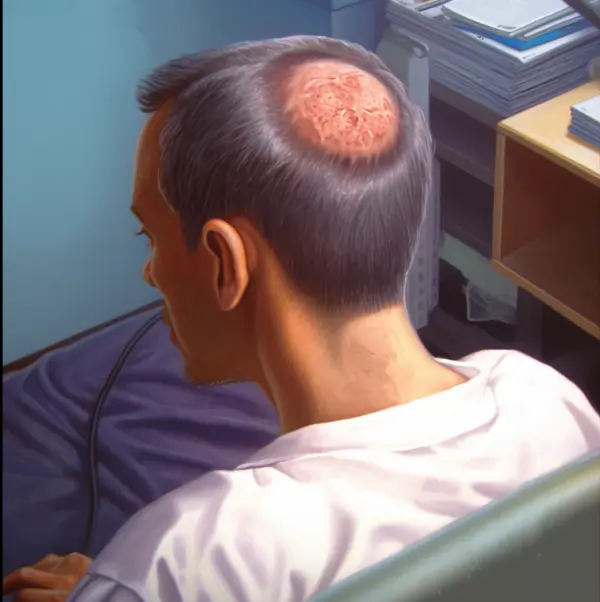
Localized hair loss: Severe or recurrent folliculitis can lead to damage to the hair follicles, resulting in hair loss in the affected areas.
The clinical course of folliculitis can be acute, chronic, or recurrent. Chronic cases are particularly challenging to manage, as they may lead to complications such as scarring or keloid formation.
Types of Folliculitis
Folliculitis can be classified into different types based on the depth of follicular involvement, the underlying cause, and the location of the lesions. The following are the most common types of folliculitis:
Superficial Folliculitis
Bacterial Folliculitis: This is the most common form of superficial folliculitis, often caused by Staphylococcus aureus bacteria. It presents as small pustules around hair follicles, typically on areas of the body prone to friction or occlusion. Poor hygiene, shaving, and tight clothing can exacerbate this condition.
Hot Tub Folliculitis: Caused by Pseudomonas aeruginosa, this form of folliculitis occurs after exposure to contaminated water in hot tubs, whirlpools, or swimming pools. Symptoms usually develop 24 to 48 hours after exposure and typically resolve on their own within a few days.
Pseudofolliculitis Barbae: Often seen in individuals who shave frequently, particularly in people with curly hair, this condition is caused by ingrown hairs that irritate the skin and lead to inflammation. It is most commonly observed on the face and neck.
Deep Folliculitis
Sycosis Barbae: This is a more severe form of folliculitis that affects deeper portions of the hair follicles. It usually presents in men who shave, leading to painful, deep-seated pustules or nodules in the beard area.
Gram-Negative Folliculitis: This type of folliculitis is often seen in individuals who have been on long-term antibiotic treatment for acne. The condition is caused by gram-negative bacteria, such as Klebsiella or Enterobacter, leading to pustules and papules on the face or upper trunk.
Boils and Carbuncles: These are deeper infections of the hair follicle, usually caused by Staphylococcus aureus. Boils (furuncles) involve a single hair follicle, while carbuncles are clusters of infected follicles. They present as painful, red, swollen areas that may drain pus.
Etiology and Pathogenesis: The pathogenesis of folliculitis involves the disruption of the normal integrity of the hair follicle, followed by the entry of microorganisms or other irritants. Several factors can contribute to this process:
Infectious Agents: Bacterial, fungal, viral, and parasitic infections are common causes of folliculitis.
Bacteria: Staphylococcus aureus is the most common bacterial pathogen associated with folliculitis. Other bacteria, such as Pseudomonas aeruginosa and gram-negative organisms, can also cause folliculitis under specific circumstances.
Fungi: Dermatophytes (fungal pathogens that infect the skin, hair, and nails) can cause a type of folliculitis known as tinea barbae, typically seen in individuals with fungal infections of the beard area. Malassezia species, which are part of the normal skin flora, can also cause folliculitis in predisposed individuals.
Viruses: Herpes simplex virus (HSV) can lead to folliculitis-like lesions, particularly in immunocompromised individuals.
Parasites: Folliculitis caused by parasites, such as Demodex mites, is less common but can occur in certain cases, especially in individuals with underlying immune deficiencies.
Mechanical Trauma: Friction from clothing, shaving, or other mechanical irritants can lead to follicular injury, allowing bacteria to invade the hair follicle. In individuals who frequently shave, ingrown hairs can exacerbate the inflammatory process, particularly in pseudofolliculitis barbae.
Occlusion and Heat: Occlusion from tight clothing or bandages, combined with heat and humidity, can promote folliculitis. The warm, moist environment encourages bacterial growth and follicular occlusion, leading to inflammation.
Immune Suppression: Immunocompromised individuals, such as those with HIV or those on immunosuppressive medications, are at higher risk of developing infectious folliculitis due to their impaired ability to fight off microbial pathogens.
Diagnosis: Diagnosis of folliculitis is primarily clinical, based on the characteristic appearance of the lesions. In most cases, a thorough history and physical examination are sufficient for diagnosis. However, sometimes additional diagnostic tests may be required as with the following situations:
Bacterial Cultures: In cases of recurrent or resistant folliculitis, bacterial cultures from pustules or abscesses may be obtained to identify the causative organism and guide antibiotic therapy.
Fungal Cultures or Biopsy: Fungal cultures or skin biopsy may be necessary in suspected cases of fungal folliculitis, especially when the lesions do not respond to conventional treatment.
Viral Cultures or PCR: In cases of suspected viral folliculitis, particularly in immunocompromised patients, viral cultures or polymerase chain reaction (PCR) testing may be performed to identify the causative virus.
Biopsy: In cases where the diagnosis is uncertain, or if the condition does not respond to standard treatments, a skin biopsy may be performed to rule out other inflammatory or neoplastic conditions.
Treatment: The treatment of folliculitis depends on the underlying cause, severity, and extent of the condition. Management strategies typically include both topical and systemic therapies, as well as lifestyle modifications to prevent recurrence.
Topical Therapy:
Antibiotics: Topical antibiotics, such as mupirocin or clindamycin, are commonly used to treat bacterial folliculitis. They are applied directly to the affected areas to reduce bacterial colonization and inflammation.
Antifungals: In cases of fungal folliculitis, topical antifungal agents such as ketoconazole or clotrimazole may be used to treat the infection.
Antiseptics: Chlorhexidine washes or benzoyl peroxide may be used to help reduce bacterial load and prevent recurrence.
Systemic Therapy:
Oral Antibiotics: For moderate to severe bacterial folliculitis or cases that do not respond to topical therapy, oral antibiotics such as doxycycline or cephalexin may be prescribed. Treatment duration is typically 7 to 14 days, depending on the severity of the infection.
Oral Antifungals: In cases of tinea barbae or severe fungal folliculitis, oral antifungal agents such as terbinafine or itraconazole may be required.
Antivirals: In cases of viral folliculitis caused by herpes simplex virus, antiviral medications such as acyclovir or valacyclovir may be used.
Lifestyle Modifications:
Hygiene: Maintaining proper hygiene, including regular cleansing of the affected areas with antiseptic washes, can help reduce the risk of recurrent folliculitis.
Avoiding Friction and Occlusion: Wearing loose-fitting clothing and avoiding activities that promote excessive friction or occlusion of the skin can reduce the likelihood of follicular irritation and inflammation.
Conclusion: Folliculitis is a common and often benign condition that can cause significant discomfort and cosmetic concerns. While superficial forms of folliculitis typically resolve on their own or with minimal intervention, deeper or chronic cases may require more aggressive treatment to prevent complications such as scarring and hair loss. Understanding the underlying cause of folliculitis is key to effective management, as bacterial, fungal, viral, and mechanical factors all play a role in its pathogenesis. By combining appropriate topical or systemic therapies with preventive measures, most cases of folliculitis can be successfully treated, allowing individuals to achieve symptom relief and improved quality of life.
Berger RS, Seifert MR. Whirlpool folliculitis: a review of its cause, treatment, and prevention. Cutis. 1990 Feb;45(2):97–8.
1.
Herman LE, Harawi SJ, Ghossein RA, Kurban AK. Folliculitis. A clinicopathologic review. Pathol Annu. 1991;26 Pt 2:201–46.
1.
Weinberg JM, Mysliwiec A, Turiansky GW, Redfield R, James WD. Viral folliculitis. Atypical presentations of herpes simplex, herpes zoster, and molluscum contagiosum. Arch Dermatol. 1997 Aug;133(8):983–6.
1.
Fearfield LA, Rowe A, Francis N, Bunker CB, Staughton RC. Itchy folliculitis and human immunodeficiency virus infection: clinicopathological and immunological features, pathogenesis and treatment. Br J Dermatol. 1999 Jul;141(1):3–11.
1.
Jang KA, Kim SH, Choi JH, Sung KJ, Moon KC, Koh JK. Viral folliculitis on the face. Br J Dermatol. 2000 Mar;142(3):555–9.
1.
Al-Dhafiri SAM, Molinari R. Herpetic folliculitis. J Cutan Med Surg. 2002;6(1):19–22.
1.
Luelmo-Aguilar J, Santandreu MS. Folliculitis: recognition and management. Am J Clin Dermatol. 2004;5(5):301–10.
Sun KL, Chang JM. Special types of folliculitis which should be differentiated from acne. Dermatoendocrinol. 2017;9(1):e1356519.
1.
Durdu M, Errichetti E, Eskiocak AH, Ilkit M. High accuracy of recognition of common forms of folliculitis by dermoscopy: An observational study. J Am Acad Dermatol. 2019 Aug;81(2):463–71.
1.
Draelos ZD. Examining 15% Azelaic Acid Foam for the Treatment of Folliculitis: A Pilot Study. J Clin Aesthet Dermatol. 2020 Apr;13(4):36–8.
1.
Starace M, Yamagata JP, Cortez de Almeida RF, Frattini S, Bruni F, Alessandrini A, et al. A Practical Algorithm for the Management of Superficial Folliculitis of the Scalp: 10 Years of Clinical and Dermoscopy Experience. Dermatol Pract Concept. 2023 Jul 1;13(3):e2023131.
Syphilis is a chronic, multistage infectious disease caused by the spirochete Treponema pallidum. Known historically as “the great imitator,” syphilis has puzzled clinicians for centuries…
Head lice (Pediculus humanus capitis) are parasitic insects that infest human scalps, feeding on blood and causing a condition known as pediculosis. This article explores…
Introduction: Kerion Celsi is a severe, inflammatory form of tinea capitis, primarily affecting children. It is characterized by a boggy, purulent, and sometimes painful lesion…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.