Trichothiodystrophy (TTD) is a rare, autosomal recessive disorder characterized by sulfur-deficient hair, developmental anomalies, and a spectrum of systemic manifestations. It falls under the category of DNA repair disorders, sharing some genetic and phenotypic overlaps with xeroderma pigmentosum (XP) and Cockayne syndrome (CS). However, TTD is distinct in its presentation and molecular underpinnings. This article aims to provide a detailed overview of TTD, focusing on its genetic basis, clinical manifestations, diagnostic approaches, and management strategies.
Genetic Basis of TTD: The hallmark of TTD lies in its genetic etiology. The disorder is primarily caused by mutations in genes encoding subunits of the transcription factor IIH (TFIIH), a multiprotein complex essential for nucleotide excision repair (NER) and transcription. The most frequently implicated genes include ERCC2 (XPD), ERCC3 (XPB), and GTF2H5 (TTDA). These mutations disrupt the normal functioning of TFIIH, impairing both the repair of UV-induced DNA damage and transcriptional activities.
Additionally, some forms of TTD are linked to defects in sulfur (European spelling: sulphur) incorporation into hair keratins. These are attributed to mutations in TTC37 and MPLKIP (also known as TTDN1), which are involved in sulfur metabolism and keratinocyte function. The resulting sulfur-deficient hair is a defining feature of the disorder.
Clinical Manifestations: TTD exhibits a wide clinical spectrum, reflecting its multisystemic involvement. While the disorder is best known for its hair abnormalities, systemic manifestations can severely impact the quality of life.
Hair Abnormalities:
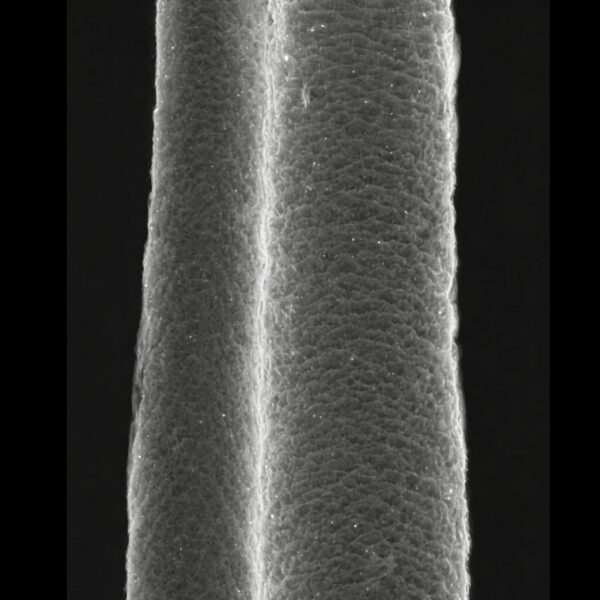
The hallmark feature of TTD is brittle, sulfur-deficient hair. This is often described as “tiger tail” hair due to its characteristic alternating light and dark bands under polarized light microscopy. Under the microscope the hair can be seen to have a squashed oval shape in cross section, an irregular diameter along its length, has abnormal or no cuticle, and with abnormal irregular pigment incorporation along its length.
Hair fragility leads to hair shaft breakage, resulting in short, sparse hair over the scalp. Alopecia is common. The hair follicles of trichothiodystrophy affected individuals are all fully functioning, but the hair is so brittle that once it emerges from the skin and becomes exposed to the environment trichorrhexis nodosa, trichoclasis, and trichoschisis occur in the hair fibers. The breakage and fracturing in the brittle hair result in the short, sparse appearance.
Neurological Features:
Intellectual disability is prevalent, ranging from mild to severe.
Motor delays, seizures, and microcephaly may also occur.
Myelin abnormalities, detected via MRI, are common and contribute to neurological deficits.
Skin and Photosensitivity:
Approximately 50% of TTD patients exhibit photosensitivity due to defective NER. This can manifest as erythema and blistering upon UV exposure.
Non-photosensitive forms of TTD are associated with mutations in non-DNA repair genes.
Growth and Developmental Abnormalities:
Prenatal and postnatal growth retardation are hallmarks.
Dysmorphic facial features, such as a prominent forehead and small chin, are common.
Reproductive and Endocrine Disorders:
Female patients may exhibit ovarian dysgenesis, leading to infertility.
Hypothyroidism and other endocrine anomalies are also reported.
Immunological and Systemic Features:
Recurrent infections due to impaired immunity are observed in some cases.
Ichthyosis and nail dystrophy are frequent dermatological manifestations.
Ocular and Skeletal Abnormalities:
Cataracts and other ocular anomalies may develop.
Skeletal abnormalities include joint contractures and osteoporosis.
Pathophysiology: The underlying pathophysiology of TTD revolves around the dual role of TFIIH in DNA repair and transcription. Mutations in TFIIH subunits lead to impaired NER, reducing the cell’s ability to repair UV-induced DNA lesions. This explains the photosensitivity observed in a subset of patients.
Simultaneously, defects in transcriptional regulation disrupt the expression of genes necessary for normal development and function. This dual impairment accounts for the systemic manifestations of TTD, including growth retardation, neurological deficits, and sulfur-deficient hair.
Notably, mutations affecting sulfur metabolism contribute to the unique hair phenotype. Sulfur is a critical component of keratin, the structural protein in hair. Sulfur-deficient keratin results in brittle, fragile hair that lacks structural integrity.
Where trichothiodystrophy is suspected in patients attending a dermatology clinic, hair samples are sometimes tested for sulfur content and cysteine amino acid content. Trichothiodystrophy affected hair has only around 50% of the sulfur and cysteine content found in normal hair.
Diagnostic Approaches: Diagnosing TTD involves a combination of clinical evaluation, laboratory investigations, and molecular genetic testing.
Clinical Evaluation:
Hair abnormalities, developmental delays, and systemic features should prompt suspicion of TTD.
Photosensitivity and characteristic facial features provide additional diagnostic clues.
Microscopic Examination:
Polarized light microscopy of hair shafts reveals the “tiger tail” pattern, a pathognomonic finding in TTD.
Elemental analysis of hair may demonstrate reduced sulfur content.
Genetic Testing:
Whole exome sequencing or targeted gene panels can identify causative mutations in TFIIH subunits or sulfur metabolism-related genes.
Genetic counseling is recommended for affected families.
Imaging and Neurodevelopmental Assessment:
Brain MRI may reveal myelin abnormalities or other structural anomalies.
Developmental assessments help quantify the severity of intellectual disability and motor delays.
Differential Diagnosis: TTD shares features with several other genetic disorders, necessitating careful differentiation:
Xeroderma Pigmentosum:
Like TTD, XP involves defective NER. However, XP is primarily characterized by severe photosensitivity, early-onset skin cancers, and less frequent systemic involvement.
Cockayne Syndrome:
CS overlaps with TTD in its photosensitivity, developmental delays, and growth retardation. However, CS patients typically lack the brittle hair seen in TTD.
Ichthyosis Syndromes:
The ichthyosis observed in TTD can resemble other forms of inherited ichthyosis. The presence of hair abnormalities helps distinguish TTD.
Other Syndromes with Brittle Hair:
Conditions such as Menkes disease and Netherton syndrome may also present with hair abnormalities but have distinct molecular and clinical profiles.
Management and Prognosis: TTD remains an incurable disorder, with management focused on alleviating symptoms and improving quality of life. Multidisciplinary care is essential, involving dermatologists, neurologists, endocrinologists, and other specialists as needed.
Dermatological Care:
Gentle hair care and avoidance of physical stress to the hair shaft are recommended.
Sunscreen and protective clothing are crucial for photosensitive patients.
Neurological and Developmental Support:
Physical, occupational, and speech therapies address motor and cognitive delays.
Seizures, if present, can be managed with anticonvulsants.
Endocrine and Metabolic Management:
Hormone replacement therapy may be needed for hypothyroidism or ovarian insufficiency.
Nutritional support addresses growth deficits.
Immunological Monitoring:
Regular monitoring for infections and appropriate antimicrobial therapy are vital.
Vaccinations should be kept up to date.
Psychosocial Support:
Psychological counseling and support groups help families cope with the challenges of TTD.
The prognosis of TTD varies widely depending on the severity of systemic involvement. While some patients lead relatively stable lives, others may experience significant disability and reduced life expectancy due to complications such as infections or neurological deterioration.
Research and Future Directions: Ongoing research into the molecular mechanisms of TTD may pave the way for targeted therapies. Advances in gene editing and RNA-based interventions hold promise for correcting underlying genetic defects. Additionally, further exploration of sulfur metabolism and keratin biology could lead to novel treatments for hair abnormalities.
Clinical trials investigating antioxidants, anti-inflammatory agents, and other supportive therapies are also warranted. Improved understanding of the genotype-phenotype correlations in TTD could enhance prognostication and personalized care.
Conclusions: Trichothiodystrophy is a complex, multisystem disorder with a characteristic presentation of brittle, sulfur-deficient hair and systemic involvement. Its basis in defective DNA repair and transcription underscores the intricate interplay between genomic stability and development. While TTD poses significant challenges for affected individuals and their families, advances in diagnostic techniques and supportive care have improved outcomes. Continued research into its molecular basis may eventually unlock new therapeutic possibilities, offering hope for this rare and challenging condition.
Gummer CL, Dawber RP, Price VH. Trichothiodystrophy: an electron-histochemical study of the hair shaft. Br J Dermatol. 1984 Apr;110(4):439–49.
1.
Gummer CL, Dawber RP. Trichothiodystrophy: an ultrastructural study of the hair follicle. Br J Dermatol. 1985 Sep;113(3):273–80.
1.
Itin PH, Sarasin A, Pittelkow MR. Trichothiodystrophy: update on the sulfur-deficient brittle hair syndromes. J Am Acad Dermatol. 2001 Jun;44(6):891–920; quiz 921–4.
1.
Sperling LC, DiGiovanna JJ. “Curly” wood and tiger tails: an explanation for light and dark banding with polarization in trichothiodystrophy. Arch Dermatol. 2003 Sep;139(9):1189–92.
1.
Liang C, Kraemer KH, Morris A, Schiffmann R, Price VH, Menefee E, et al. Characterization of tiger-tail banding and hair shaft abnormalities in trichothiodystrophy. J Am Acad Dermatol. 2005 Feb;52(2):224–32.
1.
Liang C, Morris A, Schlücker S, Imoto K, Price VH, Menefee E, et al. Structural and molecular hair abnormalities in trichothiodystrophy. J Invest Dermatol. 2006 Oct;126(10):2210–6.
1.
Faghri S, Tamura D, Kraemer KH, Digiovanna JJ. Trichothiodystrophy: a systematic review of 112 published cases characterises a wide spectrum of clinical manifestations. J Med Genet. 2008 Oct;45(10):609–21.
1.
Stefanini M, Botta E, Lanzafame M, Orioli D. Trichothiodystrophy: from basic mechanisms to clinical implications. DNA Repair (Amst). 2010 Jan 2;9(1):2–10.
Introduction: Rolled hairs are a relatively uncommon condition where hairs curl back into the skin instead of emerging straight from the hair follicle. This condition…
Introduction The emergence of more than one hair fiber from a single follicular opening in the skin is a phenomenon that garners significant interest in…
Grooved hair, or pili canaliculi, is a rare and unusual condition where hair fibers exhibit longitudinal grooves running along their length. This condition can affect…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.