Hair loss encompasses a vast array of conditions, each with unique clinical presentations, underlying pathophysiology, and therapeutic challenges. Within the domain of scarring (cicatricial) alopecias, a distinct yet subtle phenomenon often appears in otherwise bare patches on the scalp—the “lonely hair sign.” This sign denotes the presence of an isolated surviving hair, or a few hairs, in an area of extensive follicular destruction and scar formation. While frequently mentioned in discussions of pseudopelade of Brocq, the lonely hair sign can also appear in other forms of scarring alopecia, including lichen planopilaris and discoid lupus erythematosus, among others. This article will delve into the clinical importance, pathophysiological underpinnings, and utility of this intriguing phenomenon, offering an MSc-level exploration of what the lonely hair sign reveals about hair follicle biology and disease progression.
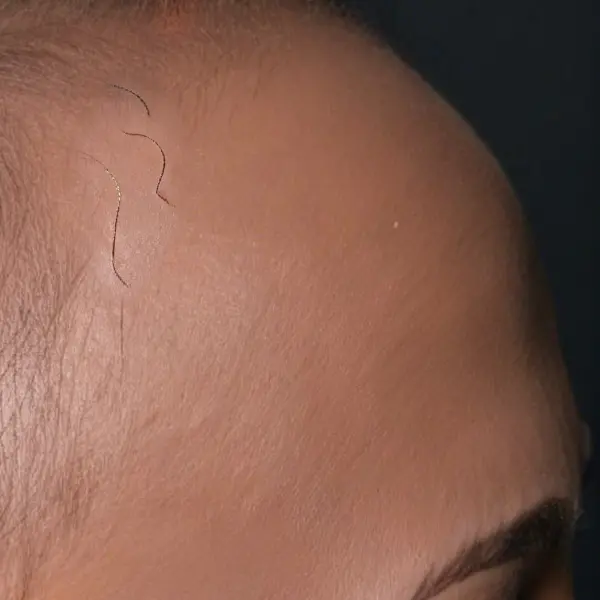
Defining the Lonely Hair Sign: The “lonely hair sign” refers to one or a few strands of hair persisting within a smooth, atrophic patch of scarring alopecia. At first glance, it can look like the hair in that solitary spot somehow evaded the inflammatory or destructive process that decimated its neighboring follicles. On scalp examination, these solitary strands stand out: they may be normal in caliber or slightly miniaturized, and they appear as “islands” of hair amidst a backdrop of tissue that no longer houses functional follicles.
The term originated from clinical observations in pseudopelade of Brocq—an enigmatic cicatricial alopecia once thought to be a standalone disorder but now often considered an end-stage manifestation of other inflammatory conditions. Nevertheless, the sign is not pathognomonic (i.e., uniquely diagnostic) of pseudopelade of Brocq and can be encountered in late-stage lesions of various other scarring alopecias.
General Overview of Scarring Alopecias: Scarring, or cicatricial, alopecias refer to a group of disorders that cause permanent hair loss through the destruction of hair follicles. In such conditions, the inflammatory process usually targets the stem cell niche within the upper follicle (isthmus) and/or the bulge region where hair follicle stem cells reside. Once these crucial stem cells are destroyed, the follicle cannot regenerate, leading to permanent alopecia and eventual replacement by fibrous (scar) tissue.
Key examples of scarring alopecias include:
Frontal Fibrosing Alopecia: A poorly understood scarring alopecia that mostly affects women. The hairline begins to recede backwards over the top of the scalp leaving a higher, larger forehead.
Lichen Planopilaris (LPP): A lymphocytic cicatricial alopecia characterized by perifollicular erythema, scale, and pruritus.
Discoid Lupus Erythematosus (DLE): A cutaneous form of lupus affecting the scalp with hyperkeratotic plaques, dyspigmentation, and eventual scarring.
Pseudopelade of Brocq: Historically described as an alopecia with minimal overt inflammation, leaving behind smooth, footprints-in-the-snow patches and, often, lonely hair strands.
Folliculitis Decalvans: A neutrophilic scarring alopecia that typically presents with pustules and crusts before leading to permanent hair loss.
In late or “burned-out” stages, these conditions may appear broadly similar – a quiet scalp devoid of active inflammation, yet characterized by areas of bare, glistening skin interspersed with occasional hair survivors. This feature sets the stage for the lonely hair sign.
Pathophysiology Behind the Lonely Hair Sign: The survival of a single hair (or a few hairs) in a region otherwise scarred raises intriguing questions about hair follicle biology and immunology. Why do these isolated hairs remain while neighboring follicles have succumbed?
Partial Immune Evasion: It is possible that some follicles elicit a weaker immune response, perhaps due to differential antigen expression. These “privileged” follicles may escape the brunt of the lymphocytic or neutrophilic attack in scarring alopecias.
Variations in Stem Cell Niche Viability: The extent of inflammation around each follicle’s isthmus and bulge can vary. In a high-intensity inflammatory milieu, most follicles lose their ability to regenerate. Follicles spared by a relatively mild inflammatory infiltration might preserve a functional stem cell population, thus remaining intact.
Disease Burn-Out: Many scarring alopecias evolve through active and quiescent phases. By the time the “burned-out” stage is reached, the destructive process has halted. If a few follicles were only mildly affected or had robust regenerative capacity, they could survive and continue producing hair.
Clinical Relevance and Diagnostic Considerations: Although commonly associated with pseudopelade of Brocq, the lonely hair sign has been documented in other forms of scarring alopecia. Clinicians, therefore, must treat it as supportive, rather than diagnostic, evidence in evaluating a patient’s condition. Some of the ways it is relevant include:
Subtle Indicator of Cicatricial Alopecia: In early or atypical cases, identifying an isolated hair shaft in a scarred patch could alert the dermatologist to the possibility of a scarring pathology rather than a nonscarring process like classical alopecia areata (which typically spares the follicular architecture, even if hairs are not visible).
Extent of Follicular Destruction: Noticing how many lonely hairs remain (or how large the scarred area is) offers clues about the severity and longevity of the disease. A broad patch containing only one or two surviving hairs typically indicates an advanced, long-standing scarring process.
Differentiation from Other Forms of Hair Loss: Non-scarring alopecias – e.g., androgenetic alopecia or classic alopecia areata – do not usually present with a shiny, atrophic patch absent of follicular ostia. In scarring alopecias, the presence of one or two hairs in a sea of smooth, fibrotic tissue sets the condition apart.
Nevertheless, scalp biopsy remains the gold standard in diagnosing scarring alopecias. Trichoscopy (dermatoscopy of the scalp) is another crucial tool that can highlight additional supportive features, such as perifollicular scale or absent follicular openings, complementing the lonely hair sign in the differential diagnosis.
Differential Diagnoses Where the Lonely Hair Sign May Appear: Since the lonely hair sign emerges in the context of follicular destruction, it is not unique to any single disorder. Dermatologists often note it in the following conditions:
Frontal Fibrosing Alopecia: A form of scarring alopecia that involves recession of the hairline backwards over the top of the scalp. Isolated hairs can be left behind in or near the original hairline.
Pseudopelade of Brocq: Long described in the literature as having subtle footprints-in-the-snow patches with minimal inflammation and isolated terminal hairs in otherwise bare areas.
Lichen Planopilaris (LPP): Though LPP typically involves more overt inflammation (perifollicular erythema, follicular hyperkeratosis), late stages can mimic pseudopelade, presenting lonely hairs in smooth areas of scarring.
Discoid Lupus Erythematosus (DLE): Hyperkeratotic plaques, dyspigmentation, and scarring characterize DLE. End-stage lesions may exhibit a few remaining follicles.
Folliculitis Decalvans: Although a neutrophilic process associated with pustules, scarring eventually leads to large bald patches. Occasionally, a few isolated hairs may survive.
From a diagnostic standpoint, the mere observation of lonely hairs is insufficient to establish a specific diagnosis. Thorough clinical assessment, trichoscopy, and scalp biopsy are necessary to characterize the pattern and cellular infiltrates, which in turn illuminate the underlying condition.
The Role of Trichoscopy: Trichoscopy, or dermoscopic evaluation of the scalp, adds critical detail to the clinical picture. When examining hair-bearing patches alongside scarred areas:
Follicular Openings: In scarring alopecias, follicular ostia disappear or are dramatically reduced in number.
Perifollicular Changes: Erythema, scale, or pigmentation around the follicle may indicate active disease.
Lonely Hair Visualization: On dermoscopy, the solitary hair shafts may be clearly visible, sometimes revealing scalp architecture changes such as the presence of fibrous tracts or “white dots” representing fibrotic tissue.
Trichoscopy helps differentiate scarring from nonscarring forms of alopecia. In classic alopecia areata, for instance, one might observe “exclamation mark” hairs or yellow dots instead of the lonely hair sign with scarring beneath. Therefore, in conjunction with the lonely hair sign, trichoscopy findings guide the diagnostic process and inform the need for biopsy in uncertain cases.
Therapeutic Implications: When a lonely hair sign is identified, the area in question has already undergone substantial follicular damage. As a result, treatment goals in scarring alopecias primarily revolve around:
Halting Progression: Using anti-inflammatory or immunomodulatory agents (e.g., topical or intralesional corticosteroids, calcineurin inhibitors, or systemic treatments like hydroxychloroquine or methotrexate) to curb ongoing inflammation.
Preserving Residual Follicles: Even a few intact follicles can be worth protecting. Reducing inflammatory insult may prevent them from being destroyed, thereby retaining some native hair.
Cosmetic Camouflage and Hair Restoration: While surgical hair transplantation in an active scarring scalp is typically discouraged, it may be considered in stable, burned-out disease. The lonely hair sign might indicate that some areas have truly “burned out,” but a specialist must confirm inactivity of inflammation via clinical and histopathological means.
Future Research and Significance: As with many nuanced signs in dermatology, the lonely hair sign highlights the need for deeper investigation into follicular immune privilege and regenerative capacity. Ongoing research in hair follicle stem cell biology aims to clarify why certain follicles survive while adjacent ones perish. Understanding these mechanisms better may unveil novel therapeutic avenues, including targeted immunomodulatory therapies, stem cell treatments, or biologics that preserve or restore follicular architecture.
Moreover, improved biomarkers to distinguish between different scarring alopecias could help refine diagnostic accuracy. For instance, identifying disease-specific cellular or molecular signatures might make it possible to differentiate lichen planopilaris from discoid lupus erythematosus at earlier stages, thus preventing further follicular destruction and preserving healthy hair. In such a future, the lonely hair sign could become less of a common clinical finding, replaced by timely detection and intervention before scarring sets in.
Conclusion: The lonely hair sign, though subtle, emphasizes significant aspects of scarring alopecias. It reminds clinicians and researchers of the complex interplay between inflammatory processes, stem cell integrity, and immune privilege within the hair follicle. While often highlighted in the context of frontal fibrosing alopecia and pseudopelade of Brocq, it does not belong to any single diagnosis and may be seen in other end-stage scarring conditions. Therefore, although it can serve as a useful clinical clue pointing to a scarring process, the lonely hair sign by itself cannot confirm a specific diagnosis – additional investigations, such as scalp biopsy and trichoscopy, are imperative.
From a patient perspective, seeing the lonely hair sign can be both hopeful and discouraging. It represents residual follicular survival amidst hairloss. Therapeutically, the focus is on arresting disease progression and conserving remaining intact follicles, since the prospect of spontaneous regrowth in scarred patches is minimal without treatment. Going forward, research that elucidates the cellular basis for selective follicular preservation could pave the way for more sophisticated, regenerative strategies to combat cicatricial/scarring alopecias. By leveraging both established clinical tools and emerging scientific insights, dermatologists and hair loss specialists strive to reduce the burden of these conditions and, eventually, make the lonely hair sign a rarer sight on the scalp.
Tosti A, Miteva M, Torres F. Lonely hair: a clue to the diagnosis of frontal fibrosing alopecia. Arch Dermatol. 2011 Oct;147(10):1240.
1.
Camacho FM. Lonely hair sign: not specific for frontal fibrosing alopecia. Arch Dermatol. 2012 Oct;148(10):1208–9; author reply 1209.
1.
Tosti A. Lonely hair sign: not specific for frontal fibrosing alopecia-reply. Arch Dermatol. 2012 Oct 1;148(10):1208–9.
1.
Dlova NC, Jordaan HF, Skenjane A, Khoza N, Tosti A. Frontal fibrosing alopecia: a clinical review of 20 black patients from South Africa. Br J Dermatol. 2013 Oct;169(4):939–41.
1.
Starace M, Brandi N, Alessandrini A, Bruni F, Piraccini BM. Frontal fibrosing alopecia: a case series of 65 patients seen in a single Italian centre. J Eur Acad Dermatol Venereol. 2019 Feb;33(2):433–8.
1.
Suchonwanit P, Pakornphadungsit K, Leerunyakul K, Khunkhet S, Sriphojanart T, Rojhirunsakool S. Frontal fibrosing alopecia in Asians: a retrospective clinical study. Int J Dermatol. 2020 Feb;59(2):184–90.
1.
Said M, El-Sayed SK, Elkhouly NDE. Trichoscopic evaluation of frontal hairline recession in Egyptian female patients. J Cosmet Dermatol. 2020 Oct;19(10):2706–16.
1.
Qiao R, Zhu J, Liu Y, Zhao X, Nie J, Lan X, et al. Refractory alopecia areata with single hairs imitating frontal fibrosing alopecia: a prospective observational study. Int J Dermatol. 2024 May;63(5):618–23.
1.
Souza GCAE, Cortez de Almeida RF, Melo DF. Trichoscopy of Frontal Fibrosing Alopecia Affecting Black Scalp: A Literature Review. Skin Appendage Disord. 2024 Oct;10(5):357–62.
1.
Quadrelli F, Cedirian S, Piraccini BM. Trichoscopy of Frontal Fibrosing Alopecia in Caucasians: A Review. Skin Appendage Disord. 2024 Dec;10(6):439–42.
Hair analysis serves as a critical tool in both clinical and research settings, enabling scientists, dermatologists, and other medical professionals to assess hair growth patterns,…
The examination of hair shafts and hair bulbs under a microscope is a critical step in diagnosing various hair disorders. A classic method to facilitate…
The hair wash test is a helpful diagnostic tool in trichology, offering clinicians and researchers a quantitative method to assess hair shedding. This test involves…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.