Hair analysis serves as a critical tool in both clinical and research settings, enabling scientists, dermatologists, and other medical professionals to assess hair growth patterns, diagnose hair disorders, and monitor the efficacy of treatments over time. Among the various techniques available for studying hair health and hair cycle dynamics, the Unit Area Trichogram (UAT) stands out for its structured, quantitative approach. This article offers a detailed exploration of what the unit area trichogram is, how it is performed, what types of information it provides, and how it compares to other hair analysis methods.
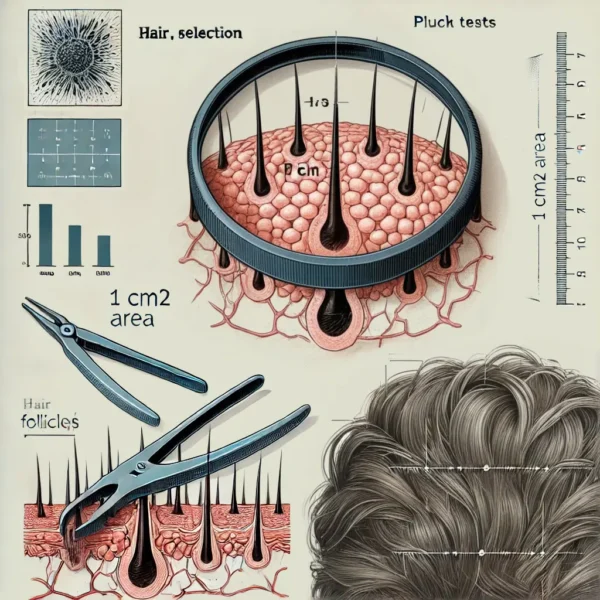
Understanding the Basics of a Unit Area Trichogram: A trichogram, in its broadest sense, is an analysis of hair that involves examining the morphology and growth-phase distribution (anagen, catagen, or telogen) of individual hair shafts and roots. Typically, a traditional trichogram entails plucking a sample of hair, preparing the hair shafts for microscopic evaluation, and analyzing the proportion of hairs in each growth phase. By comparison, the unit area trichogram (UAT) introduces an additional quantitative component: it standardizes the sampling process by focusing on a specific, predefined area of the scalp – most commonly 1 cm².
This seemingly small distinction is significant. Because the UAT targets a defined, reproducible area, it allows investigators to accurately track changes in hair density, diameter, and growth-phase distribution over time. It also helps eliminate the variability that can come from arbitrary site selection, which is often a limitation in more traditional methods of hair evaluation.
Rationale Behind a Defined Unit Area: Hair growth patterns, densities, and the proportion of hair in various phases can differ from one scalp region to another. By confining the sampling site to a unit area (e.g., 1 cm²), clinicians and researchers can:
Standardize the Assessment: Repeated assessments on the same scalp region allow for more accurate longitudinal comparison, which is essential when monitoring disease progression or response to therapy.
Improve Reproducibility: Consistent site selection means results from different measurements can be more directly compared.
Limit Variability: Focusing on a small, precise area helps reduce variability introduced by the natural heterogeneity of scalp hair.
Procedure for Conducting a Unit Area Trichogram: The practical steps for conducting a unit area trichogram vary slightly among clinics and research settings, but several core principles remain consistent:
Site Selection
Clinicians first identify a representative area of the scalp, typically avoiding regions affected by scarring, heavy hair styling product use, or visible skin lesions.
Commonly chosen sites include the mid-scalp region (vertex) for conditions like androgenetic alopecia, or an occipital area for comparison purposes if needed.
Preparation
The area of the scalp (often 1 cm²) is measured and marked carefully, often using a standard plastic or metal template.
The hair within this boundary may be clipped to a uniform length, usually close to the scalp surface, though some protocols involve plucking the hairs outright (but plucking is typically more common in classic trichograms, and less so in every UAT protocol).
Hair Collection
Depending on the specific technique:
Plucking Method: A group of hairs within the marked area is grasped firmly with forceps and swiftly pulled from the scalp. This approach can provide direct information on the hair root morphology and phase but is uncomfortable for the patient and introduces a small risk of scalp irritation.
Shave or Clip and Photographic Method: A more modern approach (sometimes referred to as a phototrichogram variation) involves shaving the area, waiting a certain number of days, then taking standardized magnified photographs to quantify regrowth. This technique is less invasive but involves slight modifications for a pure UAT approach.
Slide Preparation and Microscopic Examination (if plucking is used)
Hairs are laid out on a microscope slide, typically aligned to maintain consistent orientation (the root ends oriented in the same direction).
The proximal ends (hair roots) are examined under a microscope, sometimes after applying a clarifying medium or dye that aids in visualizing morphological details.
Data Recording
Growth Phase Distribution: The proportion of hairs in anagen, catagen, and telogen are noted.
Hair Shaft Diameter: If relevant, shaft diameter can be measured under the microscope or by using digital image analysis software.
Hair Density: The number of hairs per cm² in the examined region is recorded and can be used for longitudinal comparisons over time.
Documentation
High-resolution photographs or digital scans of the hair samples and scalp area are often archived for future reference.
Consistent time intervals between repeated assessments are crucial for meaningful data comparisons, especially in clinical trials or long-term patient monitoring.
Information Gained from the Unit Area Trichogram: One of the greatest strengths of the UAT is the broad range of data that can be collected, and the high specificity tied to a defined scalp region. Key parameters include:
Hair Density: By focusing on a 1 cm² region, clinicians can precisely calculate how many hairs grow per square centimeter of scalp. This figure is invaluable for tracking conditions like androgenetic alopecia (common pattern hair loss), telogen effluvium, or other diffuse hair loss disorders.
Anagen-to-Telogen Ratio: Determining the proportion of hair follicles in the anagen phase (active growth) relative to those in telogen (resting phase) can highlight the underlying pathology of hair loss. For instance, in telogen effluvium, the proportion of telogen hairs is abnormally high.
Hair Shaft Diameter: Evaluating the average shaft diameter helps assess miniaturization, a hallmark of androgenetic alopecia, as well as the impact of various treatments aimed at thickening hair fibers.
Morphological Clues: Abnormalities such as broken hairs, dystrophic roots, or signs of inflammation may be visible. These morphological clues can guide differential diagnoses (e.g., traction alopecia, trichotillomania, or various scarring alopecias).
Response to Treatment: By repeating the UAT periodically, clinicians can track improvements or deteriorations in hair density, caliber, and growth phase distribution after therapies such as topical minoxidil, oral finasteride, platelet-rich plasma (PRP) injections, or low-level laser therapy (LLLT).
Advantages of the Unit Area Trichogram Over Other Methods: There are several established approaches to hair analysis – such as the classic pluck trichogram, the phototrichogram, the scalp biopsy, and the wash test – among others. Each method has unique strengths and limitations. Compared to these techniques, the unit area trichogram offers notable advantages:
Standardized Sampling: Because the UAT is anchored to a specific scalp area, it provides more reproducible data over time. This is especially important for longitudinal studies, where consistent sampling is paramount for detecting subtle changes.
Non-Invasive or Minimally Invasive Options: While the pluck-based trichogram does entail some patient discomfort, certain modern UAT-based protocols (often employing photography and shaving rather than plucking) are relatively painless and more patient-friendly.
Quantitative Precision: Classical trichograms sometimes rely on arbitrary sample sizes, whereas the UAT focuses on a fixed area—ensuring that changes in hair count or density can be recorded with greater accuracy.
Better for Diffuse Hair Loss Assessment: Diffuse thinning often requires precise quantification over a defined region. The UAT captures subtle changes in density and anagen-to-telogen ratio that might be missed or under-reported in less standardized methods like the wash test (where one counts shed hairs collected after washing).
Potential for Digital Integration: Images of the specific unit area can be subjected to computerized analysis, yielding objective, repeatable metrics that reduce the risk of operator bias.
Limitations and Challenges of the UAT: Despite its many advantages, the unit area trichogram does have limitations:
Skill-Dependent Consistency: Marking the exact same 1 cm² region for repeat measurements requires skill and meticulous documentation (e.g., using tattoos, permanent scalp marks, or precise distance measurements from anatomical landmarks). Any slight shift in location may skew results.
Patient Compliance: Especially in methods involving plucking hair, patient discomfort can reduce compliance for long-term follow-ups. Additionally, hair styling routines (e.g., coloring, perming) might need to be paused or standardized to ensure reliable readings.
Time and Resource Intensive: Conducting the UAT properly involves careful site preparation, photography or plucking, microscopic analysis, and data management. It may not be ideal in fast-paced clinical settings where time and resources are limited.
Observer Bias: If the hair root classification (anagen, catagen, telogen) is done manually, it may involve some subjective assessment. Training and experience are crucial to minimize inter-observer variability.
Not Always Suitable for Focal or Scarring Alopecias: In cases of patchy or scarring alopecia, the typical target regions used for UAT may not reflect the full extent of disease if the involvement is very localized or if the scalp surface is irregular.
Comparison with Other Hair Analysis Techniques: To fully appreciate the place of the unit area trichogram in the diagnostic and research toolkit, it is helpful to understand how it stacks up against common alternatives:
Classic Trichogram: Traditionally involves plucking 50–100 hairs from various regions of the scalp to assess root morphology. While it provides similar morphological data, it lacks the standardized “unit area” aspect, making it more prone to sampling error and reduced reproducibility.
Phototrichogram: Uses photography of trimmed/scanned scalp areas over time. This method can be integrated with the UAT concept, as a phototrichogram can be conducted within a standardized 1 cm² region. One advantage of a phototrichogram is the avoidance of mechanical hair plucking, which reduces patient discomfort.
Scalp Biopsy: Provides comprehensive histological information, including follicular counts per mm², inflammatory cell presence, and other histopathological clues. However, a biopsy is invasive, can be painful, and may lead to scarring. Therefore, it is usually reserved for complex or ambiguous cases.
The Wash Test: Involves collecting shed hairs during a standardized wash process, then counting and analyzing these hairs microscopically. Although non-invasive and simple, the wash test lacks precise control over which follicles shed hairs and thus can be more variable.
Practical Applications and Clinical Utility: The unit area trichogram has found utility in a range of settings:
Research Studies on Hair Loss Treatments: Because of its precise quantification of hair density and growth phases, the UAT is used in clinical trials evaluating new drugs, topical agents, or laser devices aimed at promoting hair growth.
Monitoring Disease Progression: For patients diagnosed with androgenetic alopecia, telogen effluvium, or other diffuse hair loss conditions, periodic UAT measurements can reveal changes in hair count, shaft thickness, or growth-phase ratio, providing actionable feedback for adjustments in therapy.
Differential Diagnosis: Although not always the first step, the UAT can provide clarity when there is doubt about whether hair shedding is due to acute telogen effluvium, early androgenetic alopecia, or even combined patterns of loss.
Patient Education: Quantitative data from the UAT can be used to educate patients. Showing a visual record of hair count or density fluctuations can help explain why certain treatments may take weeks or months to exhibit measurable results.
Conclusion: The unit area trichogram represents a refined, quantitative adaptation of the classical trichogram, centered around the crucial practice of sampling from a precisely defined region of the scalp. This method offers clinicians and researchers detailed insights into hair density, growth-phase distribution, and morphological features of hair shafts and roots—while boosting reproducibility through consistent site selection and standardized procedures. Despite certain limitations, such as the need for trained personnel, potential patient discomfort (if plucking is used), and care in demarcating the target region, the UAT remains a pivotal tool in both clinical practice and hair research.
Compared to other methods of hair analysis, the UAT strikes a balance between invasiveness and diagnostic yield. It excels in monitoring diffuse hair loss over time, provides quantitative feedback for evaluating treatment outcomes, and can be integrated with modern digital imaging technologies for robust, longitudinal analyses. Especially in conditions like androgenetic alopecia or diffuse telogen effluvium, where subtle shifts in the proportion of active (anagen) follicles drive changes in scalp coverage, the precision of the UAT can be indispensable.
In sum, the unit area trichogram has become a mainstay in the repertoire of hair assessment techniques, affording standardized, reproducible, and detailed insights that benefit both patient care and scientific inquiry. By focusing on an established, reproducible unit area, clinicians can track nuanced changes in hair growth and implement more targeted, evidence-based approaches to diagnosing and managing hair disorders. As technology evolves, the integration of digital image analysis and automated counting methods into unit area trichogram protocols will likely improve consistency, reduce examiner bias, and further cement the UAT as an essential procedure in the field of hair biology.
Rushton H, James KC, Mortimer CH. The unit area trichogram in the assessment of androgen-dependent alopecia. Br J Dermatol. 1983 Oct;109(4):429–37.
1.
Rushton DH, Ramsay ID, James KC, Norris MJ, Gilkes JJ. Biochemical and trichological characterization of diffuse alopecia in women. Br J Dermatol. 1990 Aug;123(2):187–97.
1.
Rushton DH, Ramsay ID, Norris MJ, Gilkes JJ. Natural progression of male pattern baldness in young men. Clin Exp Dermatol. 1991 May;16(3):188–92.
1.
Rushton DH, de Brouwer B, de Coster W, van Neste DJ. Comparative evaluation of scalp hair by phototrichogram and unit area trichogram analysis within the same subjects. Acta Derm Venereol. 1993 Apr;73(2):150–3.
1.
Hillmann K, Blume-Peytavi U. Diagnosis of hair disorders. Semin Cutan Med Surg. 2009 Mar;28(1):33–8.
1.
Dhurat R, Saraogi P. Hair evaluation methods: merits and demerits. Int J Trichology. 2009 July;1(2):108–19.
1.
Guarrera M. Additional methods for diagnosing alopecia and appraising their severity. G Ital Dermatol Venereol. 2014 Feb;149(1):93–102.
Navigating the Complex World of Dermatology Hair Consultations: Dermatology is a medical field that deals with the health of the skin, nails, and hair. Among…
Hair breakage can be as distressing for patients as hair loss, yet the two phenomena have very different aetiologies, prognoses and management strategies. Sabouraud’s sign,…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.