Androgenetic alopecia, commonly known as male or female pattern hair loss, or pattern baldness, is a prevalent condition affecting millions worldwide. The bloodstream supplies hair follicles over the entire scalp and body. Androgen hormones, particularly testosterone, are the drivers of pattern hair loss and androgen hormones circulate throughout the entire body in the blood. However, hair loss is predominantly restricted to the top of the scalp, hair elsewhere is largely unaffected, so why is this the case? Understanding this phenomenon requires delving into the developmental biology of hair follicles, the role of androgens, and the intricate cellular and molecular mechanisms that govern hair growth and loss.
Embryological Development and Hair Follicle Predestination: During embryonic development, hair follicles are programmed to respond to androgens in a specific manner. This predestination is a critical factor in determining whether a hair follicle will miniaturize and cease to produce visible hair or grow robustly in response to androgens, or have no significant response. This intrinsic property of hair follicles is evident from the outcomes of hair transplantation procedures. Hair follicles transplanted from the back of the scalp, which are typically resistant to androgen-induced miniaturization, continue to grow in their new location on the top of the scalp. Conversely, follicles from the top of the scalp transplanted to other regions retain their predisposition to miniaturize in response to androgens.
Very early on during embryonic development different groups of cells are directed towards making different parts of the body and different areas of skin. The cell group that makes the skin and hair follicles on top of the scalp is different from the cell population that makes the skin and hair on the sides and back of the scalp. It seems that the cells that make the scalp skin and hair on top are genetically programmed to make hair follicles that are androgen sensitive. Other distinct cell populations go on to make other regions of skin and body hair, whether it’s pubic hair, chest hair, or leg hair, etc. Each region of skin and hair has its own somewhat different characteristics. So far scientists have not found out why this androgen sensitivity occurs in only select groups of cells early in embryogenesis.
This discovery that we have distinct skin and hair follicle regions over our bodies underscores the concept that the response to androgens is an inherent characteristic of the individual hair follicles, established during embryological development. The underlying cellular and molecular mechanisms that make some hair follicles susceptible to androgens involve the number and sensitivity of androgen receptors on the surface of dermal papilla cells, which are pivotal in mediating androgen action in hair follicles.
Androgen Receptors and Dermal Papilla Cells: Dermal papilla cells, located at the base of the hair follicle, play a key role in hair growth regulation. These cells possess androgen receptors, which bind to circulating androgens such as testosterone and dihydrotestosterone (DHT). The number and sensitivity of these receptors vary between different types of hair follicles and across different body regions. For instance, dermal papilla cells from pubic hair follicles exhibit a higher density of androgen receptors compared to those from scalp hair follicles. This differential receptor expression partially explains why hair growth patterns differ between body regions in response to androgens.
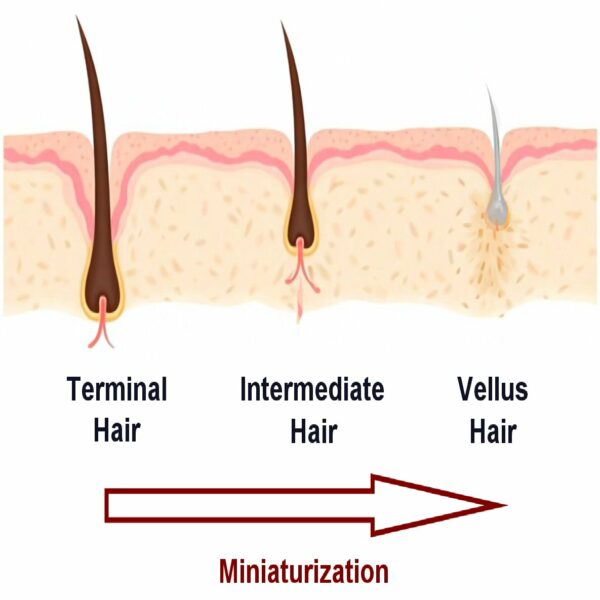
In androgenetic alopecia, hair follicles on the top of the scalp have a higher sensitivity to DHT, leading to a progressive shortening of the anagen (growth) phase and eventual miniaturization of the hair shaft. Conversely, hair follicles on the back and sides of the scalp are relatively less sensitive to androgens, allowing them to maintain normal growth cycles.
The Paradox of Androgen Action on Hair Follicles: Interestingly, the same androgens that induce hair loss on the scalp can promote hair growth in other body regions. This paradox is illustrated by the differing responses of body hair, beard hair, and scalp hair to androgens. In males, androgens stimulate the growth of beard and body hair during puberty, while simultaneously initiating the miniaturization of scalp hair follicles in genetically predisposed individuals.
The differential response is attributed to variations in the androgen receptor density, the local microenvironment of the hair follicle, and the influence of other signaling pathways. For example, while androgens can shorten the anagen phase in scalp hair, they can prolong it in body hair, leading to increased hair growth. Additionally, the effect of androgens on hair follicles can change with age. Puberty triggers the development of pubic and axillary hair, but the growth rate of these hairs declines when people are in their twenties and older. Conversely, chest hair growth peaks in mens’ forties and fifties under androgen influence.
Molecular Mechanisms and Genetic Factors: The molecular mechanisms underlying androgen action on hair follicles involve a complex interplay of genetic, hormonal, and environmental factors. Key molecular players include the enzyme 5-alpha-reductase, which converts testosterone to the more potent DHT, and various signaling pathways that modulate hair follicle cycling and apoptosis. While some 5-alpha-reductase is active in tissues away from the skin, 5-alpha-reductase can also be found locally in skin and hair follicles. Notably, higher levels of 5-alpha-reductase are found in skin and hair follicles on top of the scalp as compared to skin at the back and sides of the scalp. As such, less testosterone from the blood is converted to DHT in the skin on the back and sides of our heads.
As well as androgen hormone signalling, there are also antagonists of androgen activity that can also be present and interfere with androgen signalling to hair follicles. For example, skin at the back of the scalp has higher levels of an enzyme called aromatase. Aromatase converts androgens to estrogens, which can counteract the effects of androgens like dihydrotestosterone (DHT) that contribute to hair follicle miniaturization in AGA. By converting androgens to estrogens, aromatase reduces the local concentration of androgens, potentially protecting hair follicles from androgen-induced damage.
Genetic predisposition plays a significant role in determining an individual’s susceptibility to androgenetic alopecia. Variants in the androgen receptor gene and other genes involved in hair follicle biology can influence the density and sensitivity of androgen receptors, impacting how hair follicles respond to circulating androgens. Gene variants can also determine whether there will be higher or lower local expression of 5-alpha-reductase or aromatase, as well as other factors involved in androgen signalling to hair follicles. Overall, while hair follicles across our scalp may all look pretty much the same, the molecular signals and how they control hair growth are quite dissimilar in different areas of scalp skin.
Clinical Implications and Therapeutic Approaches: Understanding the localized effect of androgens on scalp hair loss has significant clinical implications. Treatments for androgenetic alopecia often target the hormonal pathway to reduce the impact of androgens on hair follicles. Common therapeutic approaches include the use of 5-alpha-reductase inhibitors, such as finasteride and dutasteride, which reduce the conversion of testosterone to DHT. Classically these treatments are given systemically, but recently several companies have been developing topical versions. Topical androgen inhibitor drug treatment give the advantages that only alopecia affected areas need to be treated, and local scalp skin application might also avoid risks of systemic side effects. Topical treatments like minoxidil can also promote hair growth by prolonging the anagen phase, although their exact mechanism of action is not fully understood. Interestingly, oral versions of minoxidil have been used for treating hair loss in recent years.
Hair transplantation remains a popular and effective treatment for androgenetic alopecia. By relocating androgen-resistant hair follicles from the back of the scalp to the balding areas, hair transplantation exploits the inherent resistance of these follicles to androgen-induced miniaturization. This approach provides a lasting solution for many patients, as the transplanted hair maintains its growth characteristics despite the presence of circulating androgens.
Conclusion: The localized nature of hair loss in androgenetic alopecia, confined primarily to the top of the scalp, is a result of the predetermined response of hair follicles to androgens established during our embryological development. The presence of androgen receptors on dermal papilla cells and the differential androgen sensitivity of hair follicles across various body regions further elucidate this phenomenon. Understanding these intricate biological mechanisms is crucial for developing effective treatments and managing hair loss in affected individuals. With improved knowledge and understanding of the diverse effects of androgens on hair follicles in different regions of the scalp and body skin, scientists should be able to develop new and improved treatments for pattern hair loss.
Ellis JA, Stebbing M, Harrap SB. Genetic analysis of male pattern baldness and the 5alpha-reductase genes. J Invest Dermatol. 1998 Jun;110(6):849–53.
1.
Ellis JA, Stebbing M, Harrap SB. Polymorphism of the androgen receptor gene is associated with male pattern baldness. J Invest Dermatol. 2001 Mar;116(3):452–5.
1.
Trüeb RM. Molecular mechanisms of androgenetic alopecia. Exp Gerontol. 2002;37(8–9):981–90.
1.
Ellis JA, Sinclair R, Harrap SB. Androgenetic alopecia: pathogenesis and potential for therapy. Expert Rev Mol Med. 2002 Nov 19;4(22):1–11.
1.
Rebora A. Pathogenesis of androgenetic alopecia. J Am Acad Dermatol. 2004 May;50(5):777–9.
1.
Inui S, Itami S. Molecular basis of androgenetic alopecia: From androgen to paracrine mediators through dermal papilla. J Dermatol Sci. 2011 Jan;61(1):1–6.
1.
Inui S, Itami S. Androgen actions on the human hair follicle: perspectives. Exp Dermatol. 2013 Mar;22(3):168–71.
Female pattern hair loss, also known as androgenetic alopecia, is a common condition typically associated with women, characterized by a diffuse thinning of hair on…
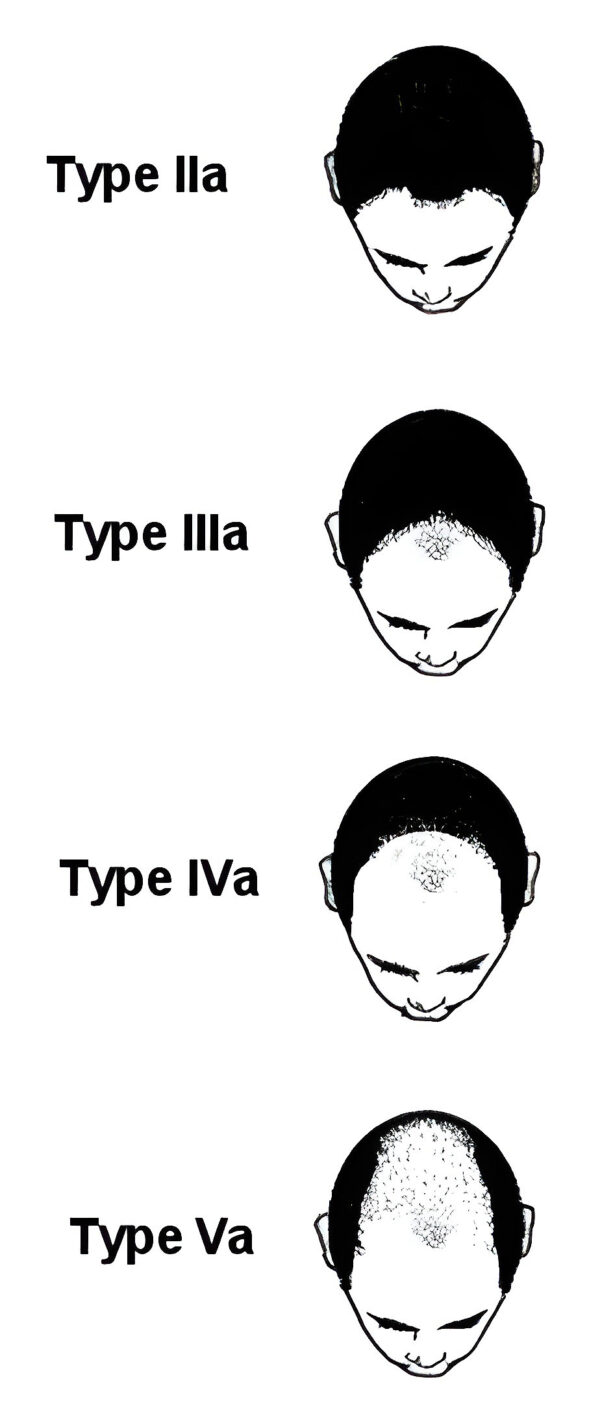
Male pattern hair loss is often diagnosed with the help of a classification system using diagrammatic representations of progressively more extensive hair loss. Originally designed…
Introduction: Androgenetic alopecia, commonly known as pattern hair loss, represents a prevalent condition affecting both men and women. It is characterized by progressive hair thinning…
Manage Cookie Consent
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.